Autonomic nervous system dysfunction, clinically termed dysautonomia, occurs when nerves controlling automatic body functions, such as heart rate, blood pressure, digestion, and sweating, stop working correctly. It affects an estimated 70 million people worldwide, with POTS alone impacting 1-3 million Americans, predominantly women aged 15-50.
Dysautonomia is misdiagnosed as anxiety or dehydration for an average of 4-6 years before correct diagnosis. This article covers types of autonomic disorders, causes, symptoms, diagnostic tests, and evidence-based treatments.
Types of Autonomic Disorders
Types of autonomic disorders span a wide spectrum. Some are manageable with lifestyle changes. Others are progressive and irreversible. Each disrupts the autonomic nervous system through a different mechanism.
Postural Orthostatic Tachycardia Syndrome (POTS)
POTS is the most common form of autonomic nervous system dysfunction in the United States. Heart rate increases by 30+ beats per minute within 10 minutes of standing, without a significant blood pressure drop. Most patients are women between 15 and 50. Many develop POTS following COVID-19 or other viral illnesses.
Neurocardiogenic Syncope
Also called vasovagal syncope, this condition triggers sudden fainting in response to prolonged standing, pain, or emotional stress. The autonomic nervous system overreacts, dropping both heart rate and blood pressure simultaneously. It is the most common cause of fainting in otherwise healthy adults.
Multiple System Atrophy (MSA)
MSA destroys autonomic nerve cells in the brainstem and spinal cord progressively. It causes severe blood pressure drops upon standing, urinary dysfunction, movement impairment, and speech changes. No cure exists. Progression occurs over 6-10 years from first diagnosis.
Pure Autonomic Failure (PAF)
PAF produces widespread autonomic nervous system dysfunction without affecting movement or cognition. Its primary presentation is severe orthostatic hypotension, the inability to maintain blood pressure when upright. PAF occurs mostly in adults over 60 and progresses slowly over years.
Types of autonomic disorders differ in severity and prognosis, but all share one defining feature: the body loses regulatory control over functions that should operate automatically.
Causes of Autonomic Nervous System Dysfunction
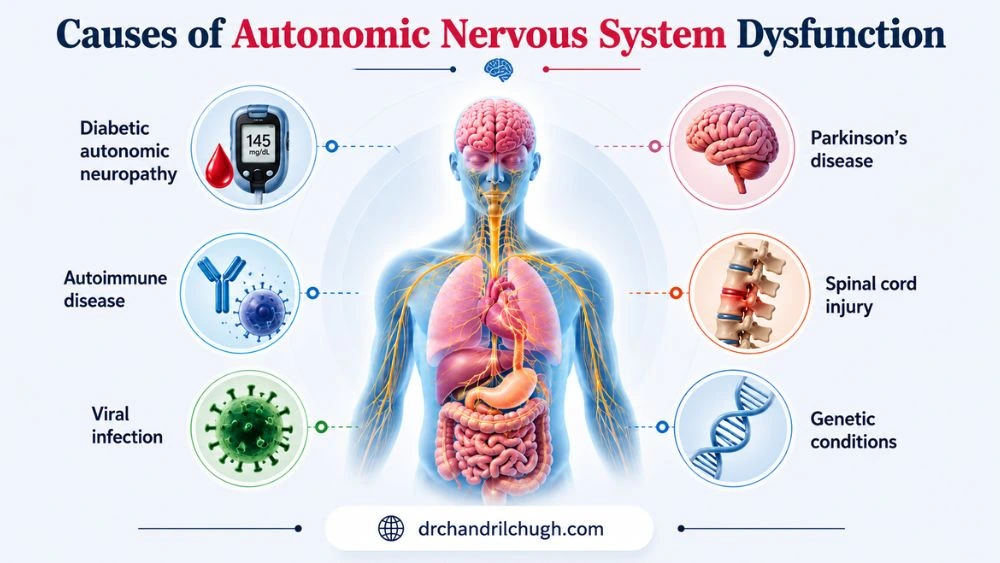
Nerve damage causing dysautonomia C is the primary biological mechanism. When peripheral nerves controlling automatic functions sustain structural damage, autonomic signals become unreliable or absent.
Key causes:
- Diabetic autonomic neuropathy : The leading cause in the United States. Persistent high blood sugar damages small autonomic nerve fibers over years. Approximately 20% of people with long-term diabetes develop clinically significant autonomic neuropathy.
- Autoimmune disease : Sjogren’s syndrome, lupus, and rheumatoid arthritis produce antibodies that directly attack autonomic nerve fibers. These are treatable causes if caught early.
- Viral infections : COVID-19, Epstein-Barr virus, and Lyme disease trigger post-infectious dysautonomia, sometimes months after the acute illness resolves. Post-COVID POTS is currently one of the fastest-growing diagnoses in US autonomic clinics.
- Chemotherapy : Vinca alkaloids (vincristine) and platinum-based drugs (cisplatin) are directly toxic to peripheral autonomic nerves.
- Parkinson’s disease : Alpha-synuclein protein deposits damage autonomic centers in the brainstem and gut wall, producing widespread dysautonomia alongside motor symptoms.
- Spinal cord injury : Disrupts descending nerve signals that regulate blood pressure and heart rate below the injury level.
- Genetic conditions : Ehlers-Danlos syndrome (hypermobile type) and familial dysautonomia (Riley-Day syndrome) carry inherited autonomic nerve dysfunction.
Causes of autonomic nervous system dysfunction frequently go unidentified for years. A diabetic patient presenting with dizziness and rapid heart rate is often treated for dehydration repeatedly before the autonomic connection is made.
Nerve damage causing dysautonomia in autoimmune cases is sometimes reversible with early immunotherapy. In degenerative forms like MSA, the damage is permanent and progressive.
Rapid Heart Rate in Autonomic Dysfunction
The autonomic nervous system balances two opposing signals: the sympathetic system accelerates heart rate, and the parasympathetic system slows it. In autonomic nervous system dysfunction, this balance fails.
In POTS specifically, standing causes blood to pool in the lower limbs. The body fails to constrict blood vessels properly to push blood back upward. The heart then accelerates aggressively to maintain cardiac output, sometimes reaching 120-150 beats per minute within minutes of standing.
Rapid heart rate autonomic dysfunction in POTS is positional. Heart rate rises with standing and drops with lying down. This distinguishes it from primary cardiac arrhythmia, where heart rate elevation is not position-dependent. Standard antiarrhythmic medications without autonomic context often worsen these patients by dropping blood pressure further.
A 2019 study published in Heart Rhythm found that POTS patients average 11 physician visits before receiving a correct diagnosis, with rapid heart rate frequently attributed to anxiety or deconditioning instead.
Rapid heart rate autonomic dysfunction also appears in early MSA before orthostatic hypotension becomes the dominant clinical problem, complicating early differential diagnosis.
Core Symptoms Across Body Systems
Autonomic nervous system dysfunction disrupts multiple body systems simultaneously. This multi-system presentation is the strongest clinical signal separating dysautonomia from single-organ disease.
Cardiovascular:
- Dizziness and lightheadedness when standing (orthostatic hypotension)
- Rapid or pounding heart rate, especially upright
- Fainting or near-fainting episodes
- Blood pressure swinging between very high and very low within the same day
Gastrointestinal:
- Gastroparesis: the stomach empties too slowly, causing bloating, early fullness, and nausea after small meals
- Alternating constipation and diarrhea without identifiable dietary trigger
- Difficulty swallowing from esophageal motility dysfunction
Temperature regulation:
- Inability to sweat normally (anhidrosis) or excessive sweating confined to small body areas
- Overheating easily without the normal cooling response activating
Bladder and urinary:
- Urinary retention from a bladder that does not empty fully
- Frequent nighttime urination (nocturia)
- Recurrent urinary tract infections from incomplete bladder emptying
Other:
- Dry eyes and dry mouth from reduced glandular secretion
- Erectile dysfunction in men (often the first symptom of diabetic autonomic neuropathy, appearing years before other signs)
- Pupil abnormalities, specifically slow adjustment when moving between light and dark environments
Most patients with autonomic nervous system dysfunction present with 3-5 concurrent symptoms across different organ systems. Treating each system in isolation without identifying the shared autonomic cause produces consistently poor outcomes.
Diagnosis and Testing Approaches
Routine blood work and standard cardiac exams return normal in most autonomic nervous system dysfunction cases. Specific autonomic testing is required.
Key diagnostic tests:
- Tilt table test : The clinical gold standard for POTS and orthostatic hypotension. The patient lies flat, then the table tilts to 70 degrees while heart rate and blood pressure are monitored for up to 45 minutes. A heart rate increase of 30+ bpm without significant blood pressure drop within 10 minutes confirms POTS.
- Quantitative sudomotor axon reflex test (QSART) : Measures sweat gland response to electrical stimulation, directly assessing small fiber autonomic nerve function at multiple body sites.
- Thermoregulatory sweat test (TST) : Maps which body regions produce absent or abnormal sweating, identifying the distribution of autonomic nerve damage.
- 24-hour ambulatory blood pressure monitoring : Captures pressure patterns during normal daily activity, including the nocturnal dipping pattern that is absent or reversed in autonomic failure.
- Skin punch biopsy for small fiber neuropathy : A 3mm biopsy from the lower leg measures intraepidermal nerve fiber density. Reduced density confirms nerve damage, causing dysautonomia earlier than nerve conduction studies.
- Valsalva maneuver with beat-to-beat blood pressure : Assesses heart rate and blood pressure responses to forced exhalation against resistance, revealing parasympathetic and sympathetic impairment patterns.
Nerve damage causing dysautonomia is confirmed most precisely through QSART and skin biopsy, both of which detect small fiber damage years before symptoms reach full severity.
Treatment for Autonomic Nervous System Dysfunction
Treatment for autonomic nervous system dysfunction requires matching the intervention to the specific type and underlying cause. No single treatment works universally across all forms.
Non-pharmacological (first-line for POTS and orthostatic hypotension):
- High fluid intake : 2-3 liters of water daily expands blood volume and reduces cardiovascular stress from upright posture.
- High sodium diet : 3,000-10,000 mg of sodium daily under medical supervision increases plasma volume. This directly contradicts standard heart-health advice and requires physician oversight.
- Compression garments : Waist-high stockings at 20-30 mmHg reduce venous blood pooling in the legs.
- Recumbent exercise : Swimming, rowing, and recumbent cycling build cardiovascular conditioning without orthostatic stress. This is the strongest long-term rehabilitation intervention for POTS, supported by multiple prospective trials.
- Head-of-bed elevation : Raising the bed head 10-30 degrees reduces nocturnal blood pressure surges and improves morning orthostatic tolerance.
Pharmacological:
- Fludrocortisone : Increases sodium and water retention, expanding blood volume. Widely used for POTS and orthostatic hypotension.
- Midodrine : Constricts peripheral blood vessels to raise standing blood pressure. FDA-approved specifically for orthostatic hypotension.
- Ivabradine : Reduces heart rate without lowering blood pressure; the preferred option for POTS patients who cannot tolerate beta-blockers.
- Pyridostigmine : Strengthens parasympathetic nerve signal transmission, improving heart rate variability in POTS patients.
- IVIG (intravenous immunoglobulin) : Used in confirmed autoimmune dysautonomia. A 2021 Neurology paper reported meaningful autonomic improvement in 68% of autoimmune dysautonomia patients receiving IVIG.
Treatment for autonomic nervous system dysfunction in diabetic neuropathy centers on strict long-term blood sugar control. Reversal of existing nerve damage is limited, but consistent glycemic control halts further progression.
Treatment for autonomic nervous system dysfunction in post-COVID POTS follows the same protocol as primary POTS. Most post-COVID cases show measurable improvement within 12-24 months of structured management.
FAQs
What is autonomic nervous system dysfunction?
Autonomic nervous system dysfunction occurs when nerves controlling involuntary body functions, such as heart rate, blood pressure during stroke, digestion, and sweating, stop sending correct signals. It affects 70 million people globally. POTS, the most common US form, affects 1-3 million Americans, predominantly women between 15 and 50.
Can autonomic dysfunction cause rapid heart rate?
Yes. Rapid heart rate autonomic dysfunction in POTS causes heart rate to rise 30+ beats per minute within 10 minutes of standing. Blood pools in the legs; vessels fail to compensate. Heart rate regularly reaches 120-150 bpm during routine standing, and the elevation drops immediately with lying down.
What causes damage to the autonomic nervous system?
Causes of autonomic nervous system dysfunction include diabetic neuropathy (the leading US cause), COVID-19, Sjogren’s syndrome, lupus, vincristine chemotherapy, Parkinson’s disease, and spinal cord injury. Nerve damage causing dysautonomia from diabetes affects approximately 20% of long-term diabetic patients.
Is autonomic dysfunction permanent?
Not always. Autoimmune autonomic nervous system dysfunction improves in 68% of patients receiving IVIG. Post-COVID POTS resolves significantly in most patients within 12-24 months. Multiple system atrophy is permanent and progressive. Outcome depends entirely on the underlying cause.
How is dysautonomia diagnosed?
The tilt table test confirms POTS when heart rate rises 30+ bpm within 10 minutes of tilting. QSART and skin punch biopsy confirm nerve damage causing dysautonomia at the small fiber level. Routine cardiac exams and blood work return normal in most cases, which explains the average 4-6 year diagnostic delay.
Can lifestyle changes improve autonomic symptoms?
Yes. High sodium intake (3,000-10,000 mg daily under medical supervision), 2-3 liters of daily fluid, waist-high compression stockings, and recumbent exercise directly reduce autonomic nervous system dysfunction severity. Structured recumbent exercise programs produce measurable functional improvement in POTS within 3 months of consistent adherence.
What treatments are available for dysautonomia?
Treatment for autonomic nervous system dysfunction includes fludrocortisone (blood volume expansion), midodrine (FDA-approved for orthostatic hypotension), ivabradine (heart rate control without blood pressure reduction), and IVIG for autoimmune cases. Recumbent exercise rehabilitation delivers the strongest long-term outcomes in POTS patients.
Is autonomic dysfunction life-threatening?
Rarely, but with exceptions. Multiple system atrophy reduces life expectancy to 6-10 years post-diagnosis. Severe orthostatic hypotension in elderly patients significantly raises fall and fracture risk. POTS itself is not life-threatening; however, without proper treatment for autonomic nervous system dysfunction, it severely disables most patients.
When should I see a doctor for symptoms?
See a doctor if dizziness, rapid heart rate, or fainting occur consistently upon standing; if gastrointestinal and urinary symptoms appear alongside cardiovascular symptoms; or if sweating becomes abnormal. Multi-system symptom patterns point directly to autonomic nervous system dysfunction and require specialist referral, not repeated emergency room visits for individual symptoms.
About The Author

Medically reviewed by Dr. Chandril Chugh, MD, DM (Neurology)
Dr. Chandril Chugh is a U.S.-trained, board-certified neurologist with expertise in diagnosing and managing neurological disorders, including migraines, epilepsy, Parkinson’s disease, and movement disorders. His clinical focus includes evidence-based neurological care and patient education.
All content is reviewed for medical accuracy and aligned with current neurological guidelines.



