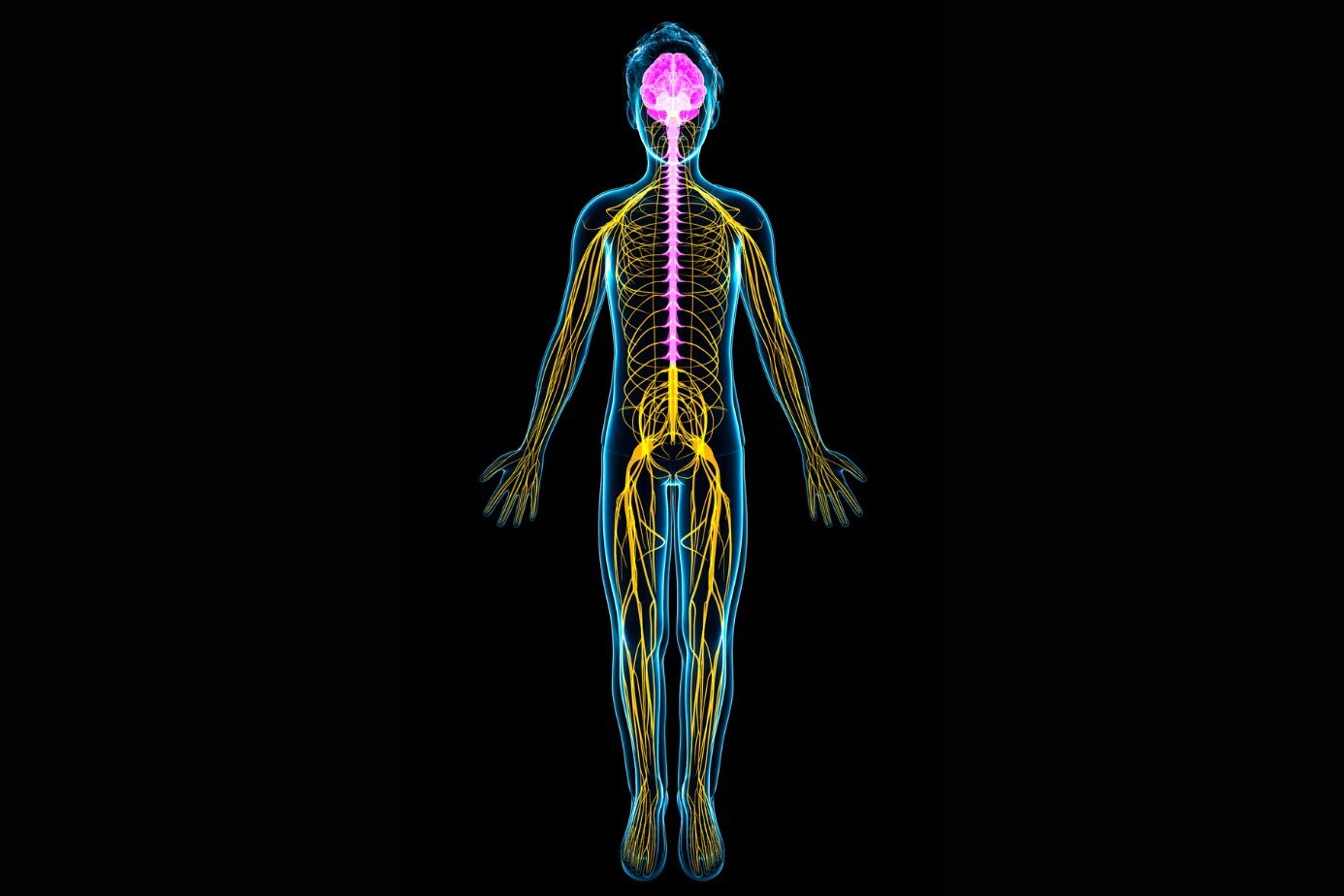
The peripheral nervous system is the network of nerves that sits outside your brain and spinal cord. It connects your brain to every muscle, organ, and patch of skin in your body. When it works, you feel, move, and breathe without thinking. When it breaks down, symptoms range from tingling feet to full muscle paralysis.
The peripheral nervous system has 43 pairs of nerves branching out to your limbs, face, chest, and gut. It gets damaged by diabetes, injury, immune attacks, toxins, and simple sustained pressure.
Most forms of damage are treatable when caught early. The ones that are not treated early often become permanent. Early nerve conduction testing, blood work, and a neurologist referral before symptoms become severe is the clearest path to full recovery.
Functions of the Peripheral Nervous System
The peripheral nervous system handles four jobs simultaneously. These jobs run in the background constantly, and most people only notice them when something goes wrong.
Sensory Function (Input to Brain)
Sensory nerves carry signals from your skin, joints, and organs to your brain. When you touch something hot, the sensory nerve in your fingertip fires a signal upward in milliseconds. Your brain reads it and responds. Without this, you would burn yourself repeatedly and not know it, which is exactly what happens in advanced diabetic neuropathy.
Motor Function (Muscle Movement)
Motor nerves carry instructions from the brain to muscles. Every deliberate movement, lifting your arm, blinking, swallowing, runs through motor nerves in the peripheral nervous system. Damage here causes weakness, paralysis, or muscle wasting.
Autonomic Regulation (Organs)
The autonomic division controls heart rate, digestion, sweating, and bladder function without conscious input. People with autonomic neuropathy from diabetes or Parkinson’s disease experience sudden blood pressure drops when standing, digestive slowdown, and abnormal sweating.
Reflex Actions
Reflex arcs bypass the brain entirely. When a doctor taps your knee with a hammer, the reflex signal travels through peripheral nerves to the spinal cord and bounces back to your muscle without brain involvement. Absent reflexes during a clinical exam indicate peripheral nerve damage.
Homeostasis Maintenance
The peripheral nervous system regulates body temperature, fluid balance, and organ function through constant low-level signaling. This is why peripheral nerve damage in critical illness patients worsens their overall stability and recovery.
Structure of the Peripheral Nervous System
Cranial Nerves
There are 12 pairs of cranial nerves. They manage face sensation, eye movement, hearing, taste, and swallowing. The vagus nerve (cranial nerve X) is the longest, running from the brainstem into the chest and abdomen to regulate heart rate and digestion.
Spinal Nerves
31 pairs of spinal nerves branch from the spinal cord. Each pair covers a specific body region. The sciatic nerve, the largest nerve in the body, forms from spinal nerves at L4 to S3 and runs down the entire leg.
Peripheral Nerve Fibers
Nerve fibers come in myelinated and unmyelinated forms. Myelinated fibers have a fatty sheath that speeds up signal transmission. Large myelinated fibers control motor function and vibration sense. Small unmyelinated fibers carry pain and temperature. This difference matters in diagnosis because some diseases attack one type and spare the other.
Neurons and Glial Cells
Neurons transmit signals. Schwann cells, the glial cells of the peripheral nervous system, wrap around axons to form the myelin sheath. When Schwann cells are damaged, nerve conduction slows. In Guillain-Barré syndrome, the immune system attacks Schwann cells directly, which causes rapid-onset paralysis.
Symptoms of Peripheral Nervous System Disorders
The symptoms of peripheral nervous system disorders vary by which nerve type gets damaged.
- Sensory nerve damage: Numbness, burning, pins and needles, loss of temperature sensing, pain that feels electric or stabbing
- Motor nerve damage: Muscle weakness, twitching, cramps, inability to lift the foot (foot drop) or wrist (wrist drop)
- Autonomic nerve damage: Dizziness when standing, constipation, irregular heartbeat, inability to sweat normally, sexual dysfunction
- Mixed damage: A combination of the above; common in diabetic neuropathy and Guillain-Barré syndrome
Symptoms starting in the feet and moving upward suggest a length-dependent neuropathy, where the longest nerves break down first. This pattern is the signature of diabetic peripheral neuropathy.
Causes of Peripheral Neuropathy
The causes of peripheral neuropathy fall into six main categories.
Diabetes (Most Common Cause)
Diabetic peripheral neuropathy affects roughly 50% of people with diabetes over their lifetime. High blood sugar damages nerve fibers directly and starves them of blood supply. The feet and lower legs go first because those nerves are the longest.
Physical Injury or Trauma
A car accident, a fall, or a sports injury can stretch, compress, or sever peripheral nerves. Radial nerve damage from a humerus fracture and sciatic nerve damage from hip dislocation are two classic examples.
Infections (e.g., Viral, Bacterial)
HIV attacks peripheral nerves through direct viral invasion and through the immune response it triggers. Lyme disease causes neuropathy in roughly 15% of untreated cases. Leprosy (Hansen’s disease) remains the leading cause of peripheral neuropathy globally in low-income countries, despite being curable.
Autoimmune Disorders
In Guillain-Barré syndrome, the immune system attacks myelin sheaths after a respiratory or gut infection. In chronic inflammatory demyelinating polyneuropathy (CIDP), this attack is slow and ongoing. Both conditions are treatable but require fast diagnosis.
Vitamin Deficiencies
Vitamin B12 deficiency causes subacute combined degeneration, where both peripheral nerves and spinal cord tracts deteriorate. Vegans and people on long-term metformin therapy (for diabetes) are at specific risk because both groups deplete B12 faster.
Toxins and Medications
Chemotherapy drugs like vincristine, paclitaxel, and cisplatin cause neuropathy in 30 to 40% of cancer patients. Chronic alcohol use damages nerves through both direct toxicity and B vitamin depletion. Heavy metal exposure (lead, arsenic, mercury) also causes peripheral nerve damage.
Injury Affecting Peripheral Nervous System
Injury affecting the peripheral nervous system follows predictable patterns depending on how the nerve gets damaged.
Compression Injuries
A nerve pressed against a bone or tight tunnel loses blood supply. Carpal tunnel syndrome compresses the median nerve at the wrist. Saturday night palsy compresses the radial nerve against the humerus during prolonged sleep in one position.
Traumatic Injuries
High-energy trauma tears or stretches nerves. Nerve injuries are graded using the Seddon classification: neurapraxia (temporary block, full recovery expected), axonotmesis (fiber damage inside intact outer sheath, slow recovery), and neurotmesis (complete severance, surgery required).
Surgical Damage
Iatrogenic nerve injury happens during otherwise routine procedures. Radial nerve injury during humeral plating surgery occurs in 2 to 5% of cases. Femoral nerve injury during hip replacement is the most common nerve complication in orthopedic surgery.
Repetitive Strain Injuries
Sustained low-level pressure over months causes cumulative nerve damage. Factory workers, musicians, and heavy computer users develop ulnar neuropathy at the elbow and median neuropathy at the wrist from repetitive motions.
Examples (Radial, Ulnar, Sciatic Nerve)
- Radial nerve: Wrist drop, weak finger extension; commonly injured in humerus fractures. A radial nerve palsy splint is the standard management tool during recovery. [See: Radial Nerve Palsy Splint : Types, Benefits, and Recovery Guide]
- Ulnar nerve: Clawing of the ring and little finger; injured at the elbow from prolonged pressure or elbow fractures
- Sciatic nerve: Pain, numbness, and weakness down the entire leg; commonly irritated by disc herniation at L4-L5 or L5-S1
How Peripheral Nervous System Disorders Are Diagnosed
Neurological Examination
The doctor tests reflexes, muscle strength, and sensation using a tuning fork, pinprick, and reflex hammer. Absent ankle reflexes with intact knee reflexes point specifically to length-dependent neuropathy.
Nerve Conduction Studies
Electrodes on the skin measure how fast electrical signals travel through a nerve. Slow conduction speed indicates myelin damage. Reduced signal amplitude indicates axon loss. These two patterns point to different diagnoses and different treatments.
Electromyography (EMG)
A needle electrode inserted into muscle detects abnormal electrical activity at rest. Fibrillation potentials (random muscle fiber discharges) confirm nerve damage to that muscle’s motor nerve. EMG separates nerve problems from muscle problems.
Blood Tests
A standard neuropathy screen includes fasting glucose, HbA1c, vitamin B12, thyroid function, and serum protein electrophoresis. The last test checks for abnormal proteins produced by blood cancers that can damage nerves.
Imaging (MRI/CT)
MRI of the spine identifies disc herniations pressing on nerve roots. MRI neurography visualizes the peripheral nerve itself, useful for locating tumors or scar tissue compressing a specific nerve.
Treatment for Peripheral Nervous System Conditions
The treatment for peripheral nervous system disorders depends entirely on cause and type of damage.
Medications for Pain Relief
- Gabapentin and pregabalin reduce nerve pain by blocking calcium channels in nerve cells
- Duloxetine (an SNRI antidepressant) is FDA-approved for diabetic neuropathic pain
- Topical lidocaine patches work for localized areas without systemic side effects
- Opioids are last-line due to tolerance and dependence risk
Physical Therapy
Therapy rebuilds strength in weakened muscles and retrains the brain to process altered sensory signals. For foot drop, ankle-foot orthoses restore walking mechanics while the nerve heals.
Nerve Repair or Surgery
Neurotmesis (complete nerve severance) requires surgical reconnection within 3 to 6 months before the target muscles atrophy irreversibly. Carpal tunnel release surgery decompresses the median nerve and produces full recovery in 85 to 90% of cases.
Lifestyle and Nutritional Support
B12 injections reverse deficiency-related neuropathy if started before permanent axon loss occurs. Stopping alcohol prevents further damage and allows partial recovery. Stopping the causative chemotherapy drug, when medically possible, also halts progression.
Managing Underlying Conditions
In diabetic neuropathy, tight blood sugar control (HbA1c below 7%) slows nerve damage progression. It does not fully reverse existing damage but prevents new damage reliably.
Can Peripheral Nerves Regenerate?
Regeneration Process
Yes. Peripheral nerves regenerate, unlike central nervous system nerves. After axon injury, the nerve stump sprouts new growth cones that follow the original nerve channel toward the target muscle or skin. This process is called Wallerian degeneration, followed by axonal regrowth.
Factors Affecting Recovery
- Age: Younger patients regenerate faster
- Gap size: Nerves separated by more than 3 cm rarely bridge the gap without surgical grafting
- Time since injury: Muscles denervated for more than 12 to 18 months lose the ability to accept reinnervation
Timeline of Healing
Peripheral nerves regenerate at roughly 1 millimeter per day, or about 1 inch per month. A radial nerve injury at the mid-humerus (about 20 cm from the wrist) takes 6 to 8 months to show functional wrist movement recovery.
Limitations of Recovery
Regenerating nerve fibers sometimes connect to the wrong targets. Motor fibers can reconnect to sensory end organs and vice versa, causing abnormal sensations or weak, misdirected movements. This is why physical therapy during recovery matters: it helps the brain remap which signals mean what.
Preventing Peripheral Nerve Damage
Blood Sugar Control
Keep HbA1c below 7% if you have diabetes. Every percentage point reduction in HbA1c reduces neuropathy progression risk by 60% based on the DCCT trial data.
Injury Prevention
Use proper lifting technique. Avoid resting elbows on hard surfaces for extended periods. Use padded handlebar grips on bicycles to prevent ulnar nerve compression in cyclists.
Ergonomic Practices
Keep wrists neutral during keyboard use. Take breaks every 30 minutes during repetitive hand tasks. Adjust chair height so elbows rest at 90 degrees without pressure on the inner arm.
Nutritional Support (B Vitamins)
B12: 2.4 mcg daily for adults; higher for vegans and metformin users. B6 deficiency causes neuropathy, but excess B6 (above 200 mg daily) also causes it. Both ends of the spectrum are harmful.
When to See a Doctor
See a neurologist if: Numbness or weakness progresses over days or weeks, symptoms affect both legs symmetrically and move upward (Guillain-Barré pattern), you have foot drop or wrist drop appearing suddenly, bladder or bowel control changes, or you have diabetes with foot numbness and no prior neuropathy evaluation. Sudden severe peripheral nerve symptoms are a medical emergency.
Frequently Asked Questions
What is the peripheral nervous system?
The peripheral nervous system is every nerve outside the brain and spinal cord. It includes 43 pairs of nerves covering muscles, skin, and organs. It handles movement, sensation, reflexes, and automatic body functions like heart rate and digestion.
Can peripheral nerves heal themselves?
Yes. Peripheral nerves regenerate at 1 mm per day. Compression injuries (neurapraxia) recover fully in 6 to 12 weeks. Injuries where the axon is damaged inside an intact sheath (axonotmesis) take 3 to 6 months. Fully severed nerves need surgery to heal.
What injuries affect the peripheral nervous system?
The most common injury affecting the peripheral nervous system includes compression (carpal tunnel, Saturday night palsy), fractures (radial nerve from humerus break, sciatic from hip dislocation), surgical damage, and repetitive strain. Fracture-related nerve injuries are the most severe because the nerve can be physically disrupted.
How are nerve disorders diagnosed?
Nerve conduction studies measure signal speed through the nerve. EMG detects abnormal muscle electrical activity at rest. Together, they confirm nerve damage, locate it, and separate myelin damage from axon loss, which directly affects treatment choice.
What is the best treatment for peripheral nervous system damage?
The treatment for peripheral nervous system damage depends on the cause. Compression injuries need splinting and time. Diabetic neuropathy needs blood sugar control plus gabapentin or duloxetine for pain. Severed nerves need surgery within 6 months. Deficiency-related neuropathy reverses with B12 injections.
Is peripheral neuropathy reversible?
It depends on the cause. Vitamin B12 deficiency neuropathy reverses fully if treated before permanent axon loss. Diabetic neuropathy stops progressing with tight sugar control but does not fully reverse. Chemotherapy neuropathy partially improves after stopping the drug. Alcoholic neuropathy improves significantly with sobriety.
When should I see a neurologist?
See a neurologist immediately if weakness or numbness spreads upward over days (possible Guillain-Barré), if you develop sudden foot drop or wrist drop, or if bladder control changes alongside limb weakness. These patterns signal conditions that worsen rapidly without treatment.
About The Author

Medically reviewed by Dr. Chandril Chugh, MD, DM (Neurology)
Dr. Chandril Chugh is a U.S.-trained, board-certified neurologist with expertise in diagnosing and managing neurological disorders, including migraines, epilepsy, Parkinson’s disease, and movement disorders. His clinical focus includes evidence-based neurological care and patient education.
All content is reviewed for medical accuracy and aligned with current neurological guidelines.